Radiation-Associated Cardiovascular & Vascular Disease
RICAD is often used as shorthand for radiation-induced coronary artery disease, but the real survivorship issue is broader: radiation can injure the heart and the blood vessels in its path. That includes the coronary arteries, carotid arteries, valves, myocardium, pericardium, conduction system, autonomic nerves, and great vessels.
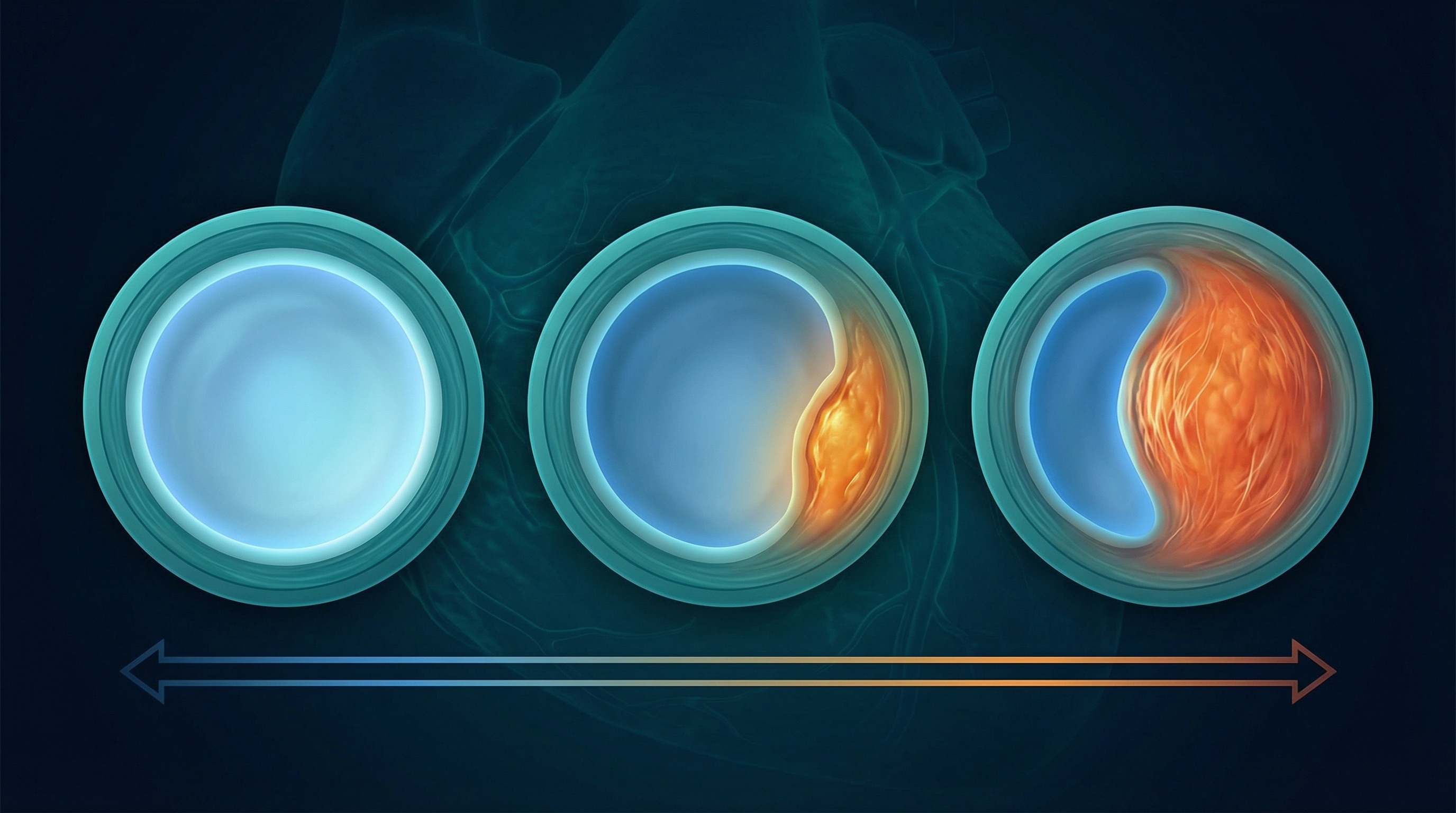
Radiation-associated plaques are often fibrotic, proximal, longer-segment, and deceptively silent compared with typical atherosclerosis. Many patients have no symptoms: radiation may also damage the nerve endings that signal chest pain. This is why screening is critical even when you feel fine.
Symptoms to Watch For
Treatment
Treatment follows conventional coronary artery disease approaches: statins, blood pressure management, stents (PCI), or bypass surgery (CABG). Catheter-based approaches are generally preferred over open surgery due to radiation-related tissue fibrosis. Earlier screening means earlier intervention.
The Full Cardiovascular Impact
Radiation and chemotherapy can damage multiple parts of the cardiovascular system, not just the coronary arteries and not just the heart muscle.
Valvular Heart Disease
Radiation causes fibrosis and calcification of heart valve leaflets: especially the aortic and mitral valves. Valvular damage is found in up to 80% of radiation heart disease patients at autopsy. Symptoms include shortness of breath, fatigue, and heart murmurs that may appear years after treatment.
Pericardial Disease
The pericardium is particularly sensitive to radiation: causing acute pericarditis, pericardial effusion (fluid buildup), or constrictive pericarditis (scarring that restricts heart movement). These can appear early or decades after treatment.
Cardiomyopathy & Heart Failure
Radiation causes myocardial fibrosis and weakening. Chemotherapy agents: particularly anthracyclines (doxorubicin) and trastuzumab: also damage heart muscle directly. Survivors who received both face compounded risk. Childhood cancer survivors treated with both had up to 61× higher cardiac disease risk.
Carotid & Vascular Disease
Neck, mantle-field, and mediastinal radiation can injure carotid and other arteries in the radiation field. Survivors may develop asymptomatic carotid plaque or stenosis years later, sometimes with longer segments and more fibrotic biology than typical atherosclerosis. This matters because carotid disease can raise stroke and TIA risk even when a survivor feels well.
Conduction System Disease
Radiation can damage the heart's electrical system, causing arrhythmias and heart block. These may require monitoring, medication, or pacemaker placement.
Autonomic Dysfunction
Radiation to the chest and neck may damage the autonomic nervous system, contributing to exercise intolerance and abnormal heart rate responses.
Screening Recommendations
When to Start Screening
The European Society of Cardiology recommends cardiovascular evaluation starting 5 years after chest radiation, then at least every 5 years: even if you feel completely fine. Radiation can damage nerve endings, masking symptoms. Don't wait for symptoms to appear.
Standard screening often includes echocardiogram and stress testing, and may include coronary CT angiography, coronary artery calcium (CAC) scoring, and carotid duplex ultrasound when the neck, mantle field, or carotids were in or near the radiation field. Talk to your doctor: ideally a cardio-oncologist: about a plan based on your specific treatment history, field, and dose.
Find a Cardio-Oncologist →Questions to Ask Your Doctor
Bring these to your next appointment. Print the page if it helps.
Were my heart, carotids, or major blood vessels in the radiation field? What dose did they receive?
Did my chemotherapy include cardiotoxic drugs (anthracyclines, trastuzumab)?
Should I get a baseline echocardiogram, stress test, coronary CT/CAC scan, or carotid ultrasound?
What is my coronary artery calcium score, and what does it mean?
How often should I be screened for cardiovascular and carotid/vascular disease?
Should I be on a statin or other preventive medication?
Should I see a cardio-oncologist? Can you refer me?
What lifestyle changes would reduce my risk the most?
Are there clinical trials or specialized programs I should know about?
What symptoms should prompt me to seek immediate care?
Key Research & Guidelines
PubMed: RICAD Research
Search published studies on radiation-induced coronary artery disease.
Search PubMedIC-OS: Find a Specialist
Searchable directory of verified cardio-oncology specialists.
Find a Doctor